Patients who have a long-standing, large rotator cuff tear may develop shoulder arthritis, also known as rotator cuff tear arthropathy. Over time, the rotator cuff tear causes abnormal shoulder motion, which gradually results in significant wear to the bony surfaces.
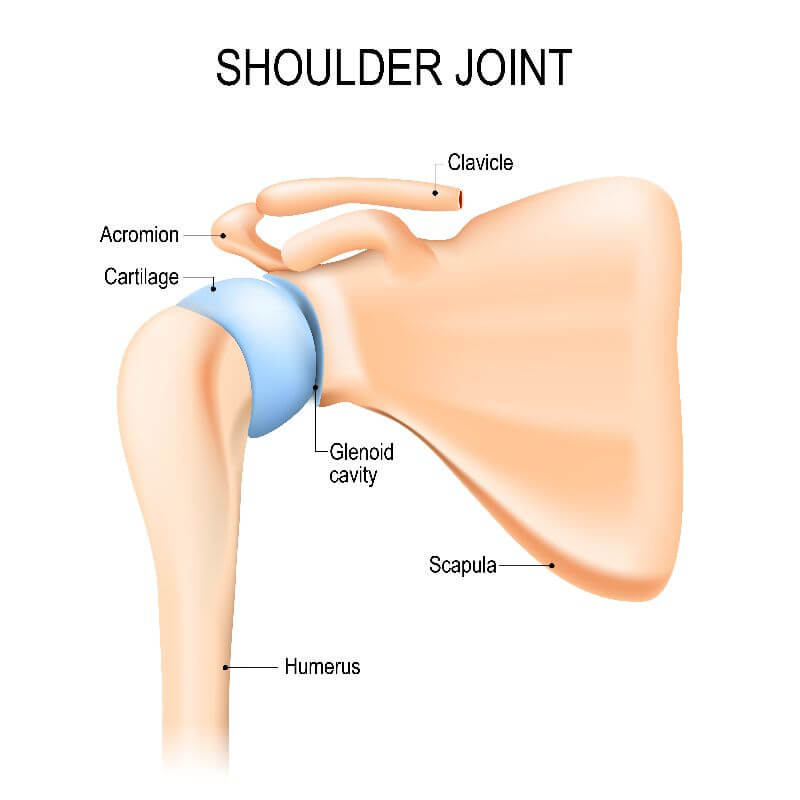
The shoulder consists of three bones, including the humerus (upper arm bone), the clavicle (collarbone), and the scapula (shoulder blade). The head of the humerus fits into the rounded socket of the scapula. This socket is called the glenoid. The point where the humeral head fits into the glenoid is called the glenohumeral joint.
The rotator cuff, a combination of muscles and tendons, keeps the humeral head centered in the glenoid. The rotator cuff tendons cover the humeral head and attach it to the shoulder blade. A second joint in the shoulder is called the acromioclavicular joint. This joint commonly has arthritis within it but usually does not require surgery for treatment.
The rotator cuff is made up of four muscles that transition into tendons.
Shoulder arthritis (or rotator cuff tear arthropathy) generally develops after a large and long-standing rotator cuff tear. The torn rotator cuff fails to hold the head of the humerus centered in the glenoid socket, and the humerus moves upward and rubs against the undersurface of the acromion. This damages the surfaces of the bones and causes arthritis to develop.
The combination of a large rotator cuff tear and advanced arthritis can lead to severe pain and weakness, and the patient may not be able to lift their arm away from their body or use their arm to lift objects.
With increasing age, the rotator cuff is more prone to tear. If a rotator cuff tear is left untreated, it may enlarge over time and progress, affecting more tendons of the rotator cuff. Such tears have a significant impact on shoulder strength and stability and cause severe shoulder pain. When the muscle is detached from the bone, shoulder strength is impaired. When the rotator cuff no longer centers the ball in the socket, stability is impaired. Consequently, the humeral head drifts upward in the socket until it abuts against the acromion bone, leading to erosion of the upper lip of the socket, and arthritis subsequently develops.
It is not fully understood why some patients develop arthritis after a rotator cuff tear, but age may be a risk factor. As we age, our tendons lose their strength, decreasing their ability to heal and regenerate. As a result, older patients with weaker tendons are more likely to develop a tear after repetitive use than younger patients whose tendons are stronger.
Symptoms of rotator cuff tear arthropathy include severe pain and poor shoulder function.
When arthritis gets worse, shoulder pain gets aggravated by use and when at rest. Night pain also becomes an issue waking patients several times during the night.
Shoulder function is affected not only by shoulder pain but also by mechanical failure of the joint where the patient cannot lift the arm away from his side and/or cannot rotate the shoulder inward or outward due to shoulder instability.
During your consultation, your orthopedic surgeon will ask you questions about your medical history and any medications you may be taking. He will also conduct a thorough physical exam. In some cases, a physical examination can immediately confirm rotator cuff tear arthropathy.
Characteristics include:
- Atrophied shoulder muscles
- Pain and grinding of the shoulder with rotational movements
- Rupture of the biceps tendon
Imaging tests such as x-rays and computerized tomography (CT) scans are useful to determine the degree of arthritis and bony relationships.
If the x-rays suggest that significant wear has occurred, a CT scan may be necessary to evaluate the shoulder further. A CT scan is a special study that provides greater detail of the bone structure and the pattern of socket wear and erosion.
Magnetic resonance imaging (MRI) scans may also be used to assess the situation further. If the ball remains centered in the socket but patients present with severe weakness of arm elevation, then an MRI is helpful to determine if there is a rotator cuff tear present that is repairable. This determination is made based on tear size, tendon retraction, and the degree of muscle atrophy.
Treatment options for rotator cuff tear arthropathy include both nonsurgical and surgical options.
Surgery is generally considered when:
- Cuff tear arthropathy results in substantial pain and loss of function that does not respond to nonsurgical treatment
- Quality of life is sufficiently impaired
- Patient is healthy, can undergo surgery, and understands and accepts the risks and alternatives.
Recommended surgical options for treating rotator cuff tear arthropathy include:
- Reverse Total Shoulder Replacement
- Shoulder Arthroscopy with Rotator Cuff and Glenohumeral Joint Debridement (Smooth and Move Procedure)
- Partial Shoulder Replacement (Hemiarthroplasty)
Like any other major surgery, shoulder replacement surgery involves certain risks such as infection, injury to nerves and blood vessels, fracture, stiffness or instability of the joint, pain, and the need for additional surgeries. There are also risks of using anesthesia.
If you suspect you have rotator cuff tear arthropathy and shoulder pain is interfering with your daily activities, call OrthoMed Center at (209) 524-4438 to schedule an appointment. You may also request an appointment online.